Are agrochemicals the cause of the Rajarata Kidney Disease?
Posted on July 18th, 2023
By Dr Parakrama Waidyanatha Courtesy The Island

Various reports in the media yet claim that the Rajarata kidney disease, scientifically defined as the chronic kidney disease of unknown etiology (CKDu), is caused by agrochemicals whereas the overwhelming evidence is that it is caused by hard water and fluoride prevalent in dug wells on high ground. Further it claimed that the number of patients is on the increase whereas published evidence is that it has been decreasing from 2016.
Agrochemicals are not the cause
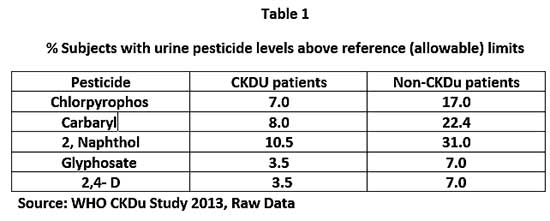
An exhaustive study carried out by the World Health Organization under the aegis of the National Science Foundation of Sri Lanka (NSF)was published in 2013. Although it failed to bring out conclusive evidence as to the etiology, it suggested an involvement of pesticides in the causation of the disease in that residues of some pesticides were above reference levels in the urine of CKDu patients. However, the pesticides residues of subjects in a non CKDu, control area (Hambantota) were also measured but the report failed to quote that data. The writer was able to get the raw data of the urine pesticide residues of Hambantota from the NSF, and to his dismay it was found that the residue levels were far higher in the urine of non-CKDu subjects of Hambantota as seen in Table 1 .As per the grapevine, the draft Report did not come up with any firm conclusions but at the insistence of the then political authority they were compelled to make some conclusions. So, it was vaguely concluded that agrochemicals probably played a role in the etiology of the disease. It is probably why the data of the non-CKDu patients were not reported!
A report entitled Health effects of fertilis ers and pesticides” was submitted to the authorities on 22-October-2021 by none other than Dr S. H. Munasinghe, Secretary, Ministry of Health. Therein he has clearly stated that there is no evidence for a direct link between the kidney disease and agrochemicals. The report may be read at: https://dh-web.org/place.names/posts/Ministry of HealthReviewAgroChem2021.pdf. (See Table 1)
There have been various other unsubstantiated claims for a link between agrochemicals and the kidney disease. For example, a research paper in an open-access (fee levying) journal, titled ‘International Journal of Public Health, Prof. Channa Jayasumana and two other authors hypothesised that glyphosate forms complexes with heavy metals such as cadmium and arsenic in hard water causing the kidney disease. No evidence has been established to prove the formation of such complexes. However, the claim that glyphosate is a probable etiolating agent led to the then government to ban glyphosate which caused serious hardships in weed management in crops. The ban was finally lifted initially for tea and later for all crops!
The claim that agrochemicals are the cause of many health problems have let to the coining of the term wasa visa to agrochemicals. It has also been purported that Sri Lanka is the country that uses the highest quantities of fertilisers and pesticides in the world! However, the available evidence as shown in Table 2 clearly establishes that Sri Lanka is one of the countries using the least amounts of both fertilisers and pesticides. (See Table 2)

Hard water and fluoride are the key causes for the disease
Not agrochemicals but fluoride and hard water are the causes for the kidney disease have been now well established. Apartment from several quality publications, a dramatic study compared two adjacent villages in Girandurukotte, namely, Badulupura, on high ground where the people exclusively drank water from dug wells and Sarabhumi in the plain where the people drank water from the river, reservoir or wells dug close to their homes. The Badulupura people contracted the disease, while affecting virtually none from Sarabhumi. Analysis of the water in the wells in the Badulupura and Sarabhumi revealed that the Badulupura water was hard and heavily contaminated with fluoride, a highly nephrotoxic chemical. However, there was no evidence of any agrochemicals above safety limits in the Badulupura waters. Further evidence for a role for fluoride in the disease is that CKD patients also often have dental fluorosis.
That people living in the planes and consuming water from reservoirs and rivers do not contaminate the disease is further exemplified by the fact that people in the Anuradhapura city and consuming tap water from the reservoirs do not contaminate the disease.
Commencing in the mid 2010-decade, community-based reverse osmosis (RO) water treatment plants were established as an interim measure for producing safe drinking water for the endemic areas of the kidney disease in the rural dry zone of Sri Lanka. It was reported that RO –treated water diminished progression of the disease. In addition, during the same period rain water harvesting and consumption were introduced to the Badulupura people, and it has now been reported there has been a diminution of the occurrence of the disease in the village. However, a formal study yet needs to be done to confirm this observation.
Moreover, a study published in the journal, Science of the Total Environment( Vol. 745, 2020) by a Japanese team of scientists in collaboration with some Sri Lankan scientists established that alkalinity, hardness and microbial parameters in the ground waters exceeded the maximum allowable limits(MAL) for drinking water in all disease affected study areas. Also, Magnesium exceeded the minimum allowable limit exclusively in the disease prevalent areas.
A further study involving feeding Wistar rats undertaken at the University of Peradeniya and reported in an issue of Ceylon Medical Journal in 2017 established that high fluoride, hard water and other undetected toxins in shallow dug wells may be the causative factor for renal and liver lesions that were detected in these rats. (Figure 01)
In vegetable growing areas of the upcountry and Puttalam where agrochemical use has been far more than in the Rajarata, no CKD has been reported. Moreover, in Mulaitive, a hard water area where no agrochemicals had been hardly used due to unavailability during the Tamil rebellion which lasted over two decades, no CKD has been reported.
Evidence is thus, overwhelming that the chronic kidney disease of unknown etiology (CKD) is related to drinking hard water containing fluoride and magnesium. Some 176,000 such wells are reported to be present in the Rajarata.
The disease in the early stages of research towards detection of its etiology was referred to it as ‘the chronic kidney disease of unknown etiology’ (CKDu). But now with a firm understanding of the cause of the disease the ‘u’ has been dropped and the disease should be referred to as the chronic kidney disease (CKD).
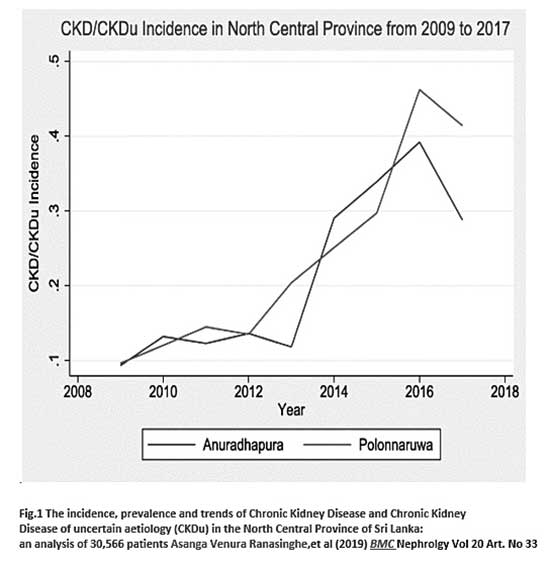
However, there are also recent claims that the numbers of CKD patients are on the increase. On the other hand the Figure 1. Clearly shows that the numbers of new patients are on the decline after the introduction of RO filters and rainwater harvesting. Regrettably, it appears that the health authorities have not published the data after 2017.
Although adequate supplies of safe drinking water may not be available in all CKD endemic areas, the people are now amply aware that the disease is caused by the consumption of hard water from wells on high ground containing fluoride and magnesium, and they avoid drinking such water.